
ACL tear is a common sports and orthopedic injury that I want to spend some time simplifying. So you just had ACL surgery or injured it and need to know everything to succeed? What is your anterior cruciate ligament (ACL) and what is its role in knee care? Who is at risk? How do I prevent an ACL tear? I have knee pain (during rehab) and years after. What is appropriate for my ACL and what should I stay away from? These are the questions I hope to shed light on. The American Physical Therapy Association has developed a Clinical Practice Guidelines that unified the information and methods of how to rehabilitate from a tear. I will add my two cents in how to bulletproof your knee and reVITALize your knee into superhuman capacity and performance. Lets delve into the technical.
How does the knee joint work?
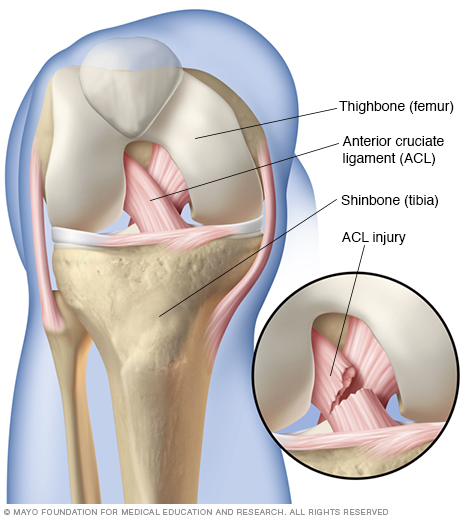
The two long bones, femur and tibia, join to make the knee joint. This complex joint looks and function like a hinge. A knee is design to straighten and bend with minimal rotation. To make this example simple, lets say the knee functions like a “true” hinge guiding a door to open and close. If you can understand this concept then you can make sense of all the nonsense out there in the internet and what advice you may hear. A knee is in a healthy position when you bend, squat, lunge, jog, and bike. All of these activities requires little to no rotation. The meniscus and knee ligaments limit the rotation. This is why our meniscus and ligaments are susceptible to aging faster. Our hips and ankle provide most of the pivoting and twisting. When we sit too much or reduce the amount of total body movement training, our body “dumbs” the impact of our hips and ankles. We have become a knee dominant society.
What is the Anterior cruciate ligament (ACL)? ACL is a ligament designed to limit the amount of twisting and hypertension movement that happens at the knee. If you cross your index and middle fingers together (middle on top) and place it on your knee, you visually see and feel the purpose of your ACL. The ACL is the middle finger where it is pointing towards your big toe. If you turn your foot inwards, like tugging on the middle finger, this “stretches” the ACL. The ligament assists in controlling the force when you move your leg. Many think you need direct contact of your knee to have a tear. A non-contact ACL tear is more common.
Who is at risk and/or risk factors?
- bad movement habits (knee collapses inwards) during simple or complex activities (running, cutting, jumping)
- weak hip musculatures especially when combine with excessive strong front thigh muscle during stepping down/squatting tasks
- previous history of ACL injury especially females (more so on the opposite leg)
- Females are 3-9 times more at risk especially during pre-Ovulation phase of the menstrual cycle
- Increased Body Mass Index (BMI)
- Decrease single leg balance
- Shoe-surface interaction
Who is at risk for re-injury?
- Improper and/or incomplete ACL knee care
- premature return to work/activities
- persistent weak front thigh (quadriceps) muscle
How do I prevent an ACL tear?
The number one biggest answer is that the thigh musculatures are not strong enough to handle to work that you need it to be done. The concept seems simple, but in under utilized in many ACL rehab. If you have been following us, strength is meaningless if your body does not know what to do with the strength. This is where we focus on functional strength, reflexive power, subconscious connection to the strength, and overload training.
There are tons of things one can do to regain the advantage of not tearing ones ACL. Multiple studies have demonstrated the value of preventative medicine. A common group that have been studied is a the female soccer teen. If you have well-structured training that addresses strengthening the hip muscle groups, core and ankle balance, proper shoe wear, good leg movement habits, and education of proper nutrition/recovery, the chances of tearing your ACL is much lower.
One overlooked aspect of preventative and rehab care in the female athlete (can apply to the male group) is internal health and well being. All females should have a regular menstruation cycle. An irregular cycle indicates malnutrition or reproductive dysfunction, both of which can be addressed with proper holistic care.
I believe the biggest reason for re-injury is due to the “new year resolution” phenomenon. Many post-ACL patients do not realize that their ACL knee care never ends. It is easy to focus your life around your ACL during your rehab and this is where people do well (unless you have improper knee care). The hardest part is to go back to school or work and juggle the foundational aspect of knee care, training for your sport/life, and deal with the rigor of life. It is tough. When one does want to work out after work, who wants to perform the basic boring stuff. Zumba, cross fit, and spinning is more fun and exciting. This is why I believe the rates of degeneration of the knee is higher after having an ACL surgery. Studies have proven the higher rates of degeneration with follow-up total knee replacement but no research has reported the why. Be disciplined and consistent on a weekly basis and you will regain the advantage. Finding a workout buddy to keep you accountable will bring consistency to your knee care.
I hope I have been able to simplify the medical jargon one might read and hear about ACL. The follow up articles will breakdown the phases of ACL so anyone can learn how take better care of their ACL no matter what stage you are in – no surgery, had recent surgery, had surgery long time ago and living a simple life or more athletic life, or had surgery but pain is still persistent. Contact us if you want us to simplify and clarify your specific ACL injury.
I pride in a comprehensive, unique, and challenging experience to ensure you never have to go through an ACL rupture. Dr Danh Ngo (I) have been helping thousands of people with knee pain and ACL rehab since 2004. As a Board Certified Sports Medicine and Orthopedic Specialist, I know you can get better.
With Gratitude,
Dr Danh Ngo